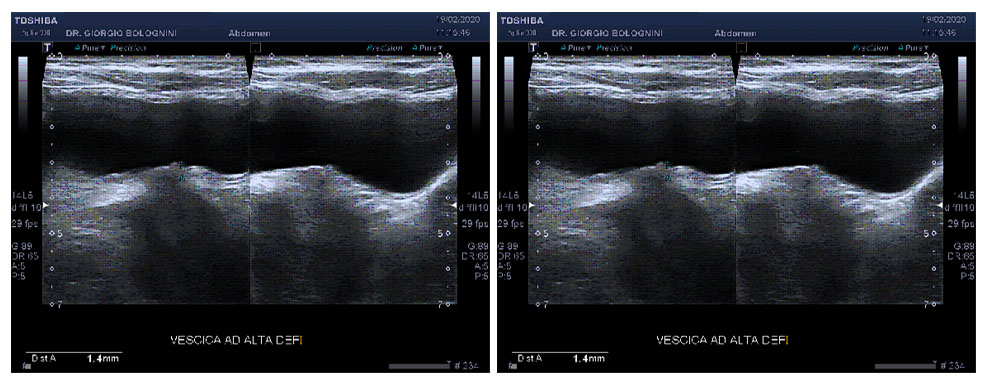
A healthy 60-year-old woman, non-smoker, two pregnancies with natural childbirth; not taking drugs regularly; in 2018 episode of subacute thyroiditis, lasting several months. In February 2020 she had an upper abdominal check-up for a right hypochondrium pain, improved with antibiotic therapy (1gr ceftriaxone for 6 days) and paracetamol. On ultrasound examination, no pathologies of the excretory biliary system were detected, with a thin choledochus of maximum 3 mm and regular alithiasic gallbladder with non-thickened walls; there were two liver microcysts. The study of the bladder with a regular Convex probe showed the presence of a thin wall eversion of the left lower side, maximum thickness 1.5mm, oval shape, which does not change position according to the patient's decubitus; the study with high frequency linear probe confirms the presence of this minimum solid wall eversion. I establish a differential diagnosis between small bladder stone attached to the wall (rear shadow cone however is not present) and micro bladder papilloma. I, therefore, recommended carrying out a diagnostic cystoscopy.
The following month, the patient performed a narcosis cystoscopy with biopsy at the Villa Donatello SpA nursing home, where the presence of solid micro-formation of the bladder fundus is confirmed; a 0.2x0.2 cm white-grey frustule is removed; in its entirety when removed.
The extemporaneous histological diagnosis is papillary neoplasm with low malignancy potential (se. WHO ISUP 2016). The patient did not have to have any type of chemo or radiotherapy treatment and carries out a six-monthly ultrasound follow-up associated with urinary cytology.