A 43-year-old woman, normal weight, came to the clinic for non-specific symptoms such as widespread abdominal swelling, particularly in the hypogastrium that had been lasting for roughly 60 days, insomnia in treatment for months with benzodiazepines, nervousness and anxiety, sporadic tachycardia, throbbing headache, night sweats and diastolic pressure rise (between 92 and 100mm\hg); intestinal tract open to faeces and gas and tractable abdomen; her case history reported 3 pregnancies with two caesarean sections and an abdominal operation for adherences in a sub-occlusive context in 1995.
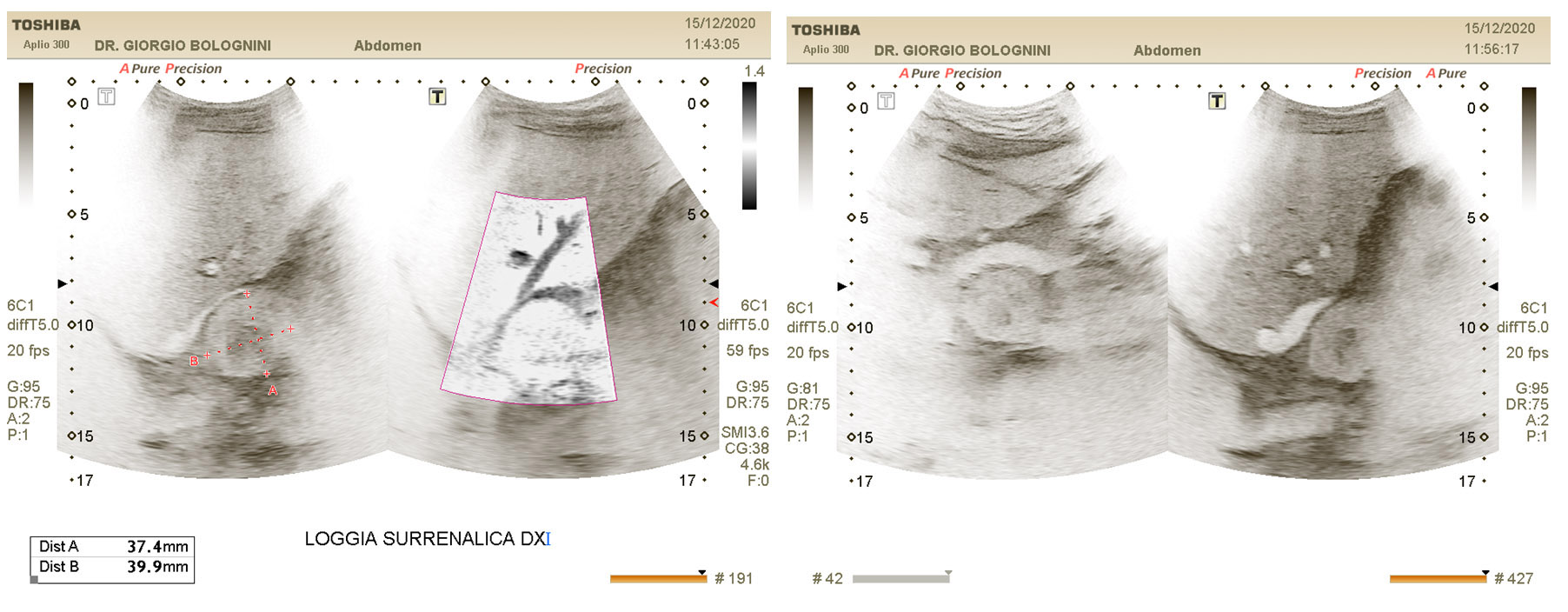
The abdominal ultrasound study identified the presence of an iso\hypoechoic nodule immediately adjacent to the right adrenal lodge of roughly 43x38mm in size, with net margins, and with end vascularization inside the Doppler SMI study. No suspicious lymphadenopathies in the peritoneal back or secondary liver metastasis of eco-perceptible size.
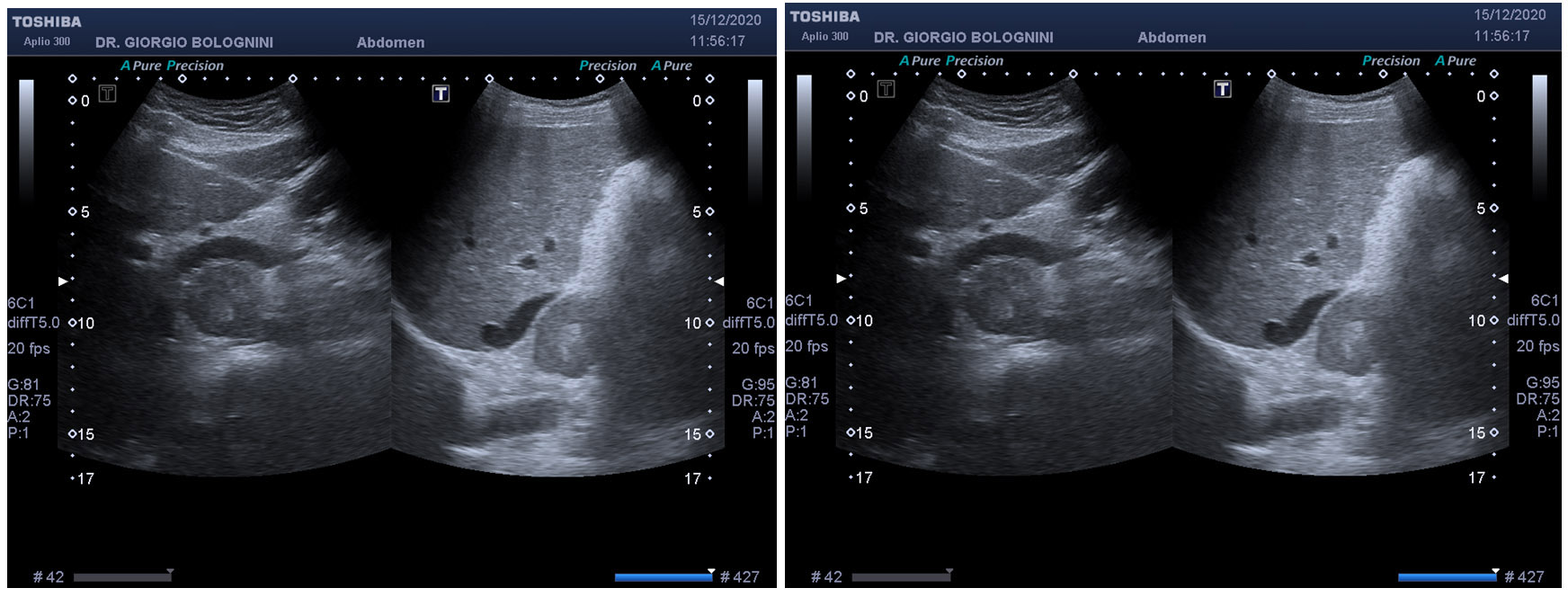
The formation was found between the aorta and the inferior vena cava (in right para-aortic), resulting in minimal compression on the left caval wall with its initial dislocation and a compression with cranialisation of the common portal trunk, the pancreatic uncinate and the first hepatic segment; posterior inferior determined compression on the left renal vein. All these retroperitoneal venous vessels were regularly free from obstructions. The formation contracted direct relationships with the first tract of the superior mesenteric artery and posteriorly with the initial tract of the right renal artery (in any case there is always present a minimal fat cleavage plane). Although not actually relevant to the adrenal lodge, I established a differential diagnosis (also based on the clinic described) between possible pheochromocytoma and extra-adrenal paraganglioma.
The subsequent contrast-enhanced abdominal CT confirmed the position and ratios of the retroperitoneal mass, describing its inhomogeneity after administration of contrast media due to the presence of areas with intense enhancement in the arterial phase and hypodense areas in all acquisition phases referrable to the central liquid\necrosis component. Presence of central calcification. The absence of hepatic secondary or locoregional evolutionary lymphadenopathies was confirmed. The urinary catecholamine dosage in the 24 hours showed a value of 65.6 of the metanephrines (normal), but of as much as 25912 of the normethanephrines.
Due to the rapid worsening (continuous tachycardia, persistent systolic diastolic hypertension in 24 hours, anxiety and manic seizures, pulsating headache and persistent vomiting) the patient was operated after circa two weeks from the CT scan result, with radical removal of the neoplastic mass in laparotomy through lower costal access, by the Prof. Luca Morelli team at the SD General Surgery 1 Univ Osp Cisanello Pisa (Director Prof. Giulio Di Candio).
The subsequent histological examination confirmed the endocrine nature of the mass, with areas of blood congestion, delimited by fibrous capsule, consisting of cellular elements with large cytoplasm, hyperchromatic nuclei and with findings of nuclear pleiomorphism, organized in nests delimited by "sustentacular" cells; immunophenotype: Synaptophysin+, Chromogranin+, CKpan-S-100 + in "sustentacular" cells; proliferation index MIB-1>3%.
The GAPP score mod. (Grading system for Adrenal Pheochromocytoma and Paraganglioma) (1,2) was as follows:
-Histological pattern (wide and irregular nests): 1
-Cellularity (high): 2
-Necrosis (absent): 0
-Capsular or vascular invasion (present): 1
-Proliferative activity (>3%): not assessable
-Catecholamine type (non-functional): not assessable
Total Score 6. The Pathological Anatomy Unit 2 of the Hospital of Pisa (director Dr V. Nardini) concluded that the set of morphological and immunohistochemical findings was compatible with moderately differentiated extra-adrenal intra-abdominal para-caval paraganglioma.
- 1. Kimura N, Takayanagi R, Takizawa N, Itagaki E, Katabami T, Kakoi N, et al. Pathological grading for predicting metastasis in phaeochromocytoma and paraganglioma. Endocr Relat Cancer. 2014;21: 405-414.
- 2. Koh JM, Ahn SH, Kim H, Kim BJ, Sung TY, Kim YH, Hong SJ, Song DE, Lee SH. Validation of pathological grading system for predicting metastatic potential in pheochromocytoma and paraganglioma PLoS One. 2017 Nov 8;12 (11): e0187398. DOI: 10.1371/journal.pone.0187398. eCollection 2017.