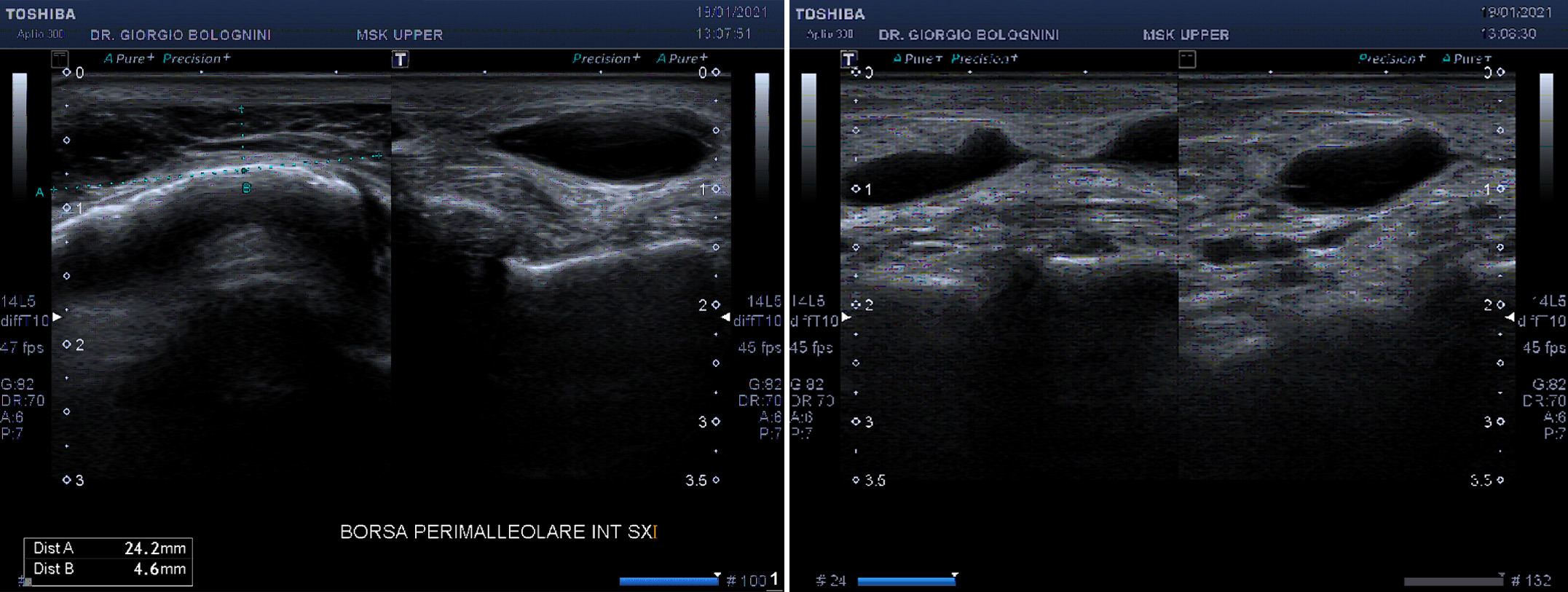
48-year-old patient, not suffering from any chronic disease and without previous major operations or of the musculoskeletal system. Wearer of safety shoes for work needs. For about 8 months she has had a substantially painless swelling in the medial compartment of her left ankle. He performs various ecocolordoppler examinations elsewhere that do not show problems relating to the deep and superficial venous circulation. The ultrasound examination performed by me shows the presence of an oval solid formation with liquid anechoic content, with a complex echo structure due to the presence of numerous internal sepimentations, of about 50x8mm, in the differential diagnosis between retromalleolar bursitis with signs of rupture and complex dermal cyst. It is associated with hyperechoic thickening of the locoregional subcutaneous and hypoechoic internal serpiginous shoots (reactive panniculitis). The tibio calcaneal ligament of the deltoid is significantly compressed by the formation, which in any case does not show coarse solutions of continuity. The posterior tibial and long flexor tendons of the fingers are also substantially within the limits. I recommend biohumoral dosages of rheumatological and thyroid markers.
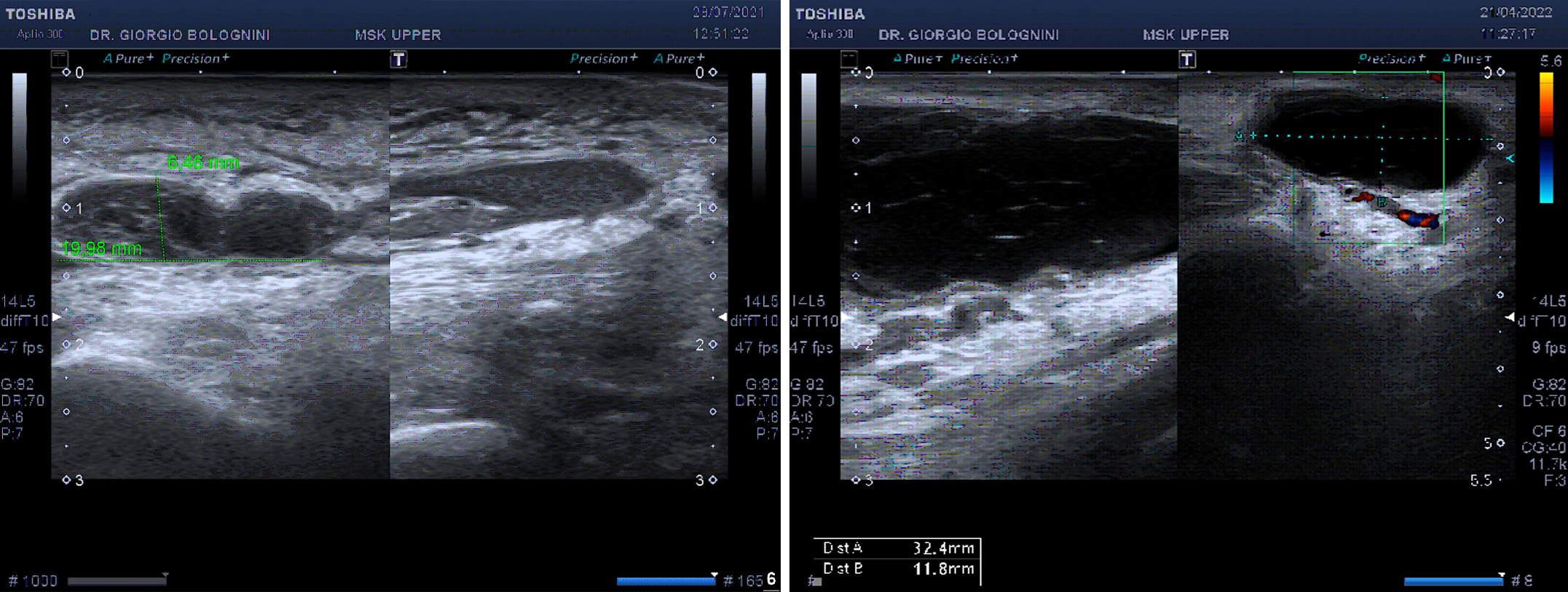
He performs an ankle MRI which confirms the presence of a large fluid sac in the soft tissues of the medial compartment of the ankle with a longitudinal extension of 60mm and a thickness of 10mm, equipped with an internal capsule and therefore compatible with a bursal distension. He performs a second ultrasound check by me after 4 months showing an increase in size of the sac and even greater evidence of internal sepimentations, with passage of the contents from simple to mixed anechoic with a level of corpuscle density in the more peripheral caudal region (similar aspect abscess); the swelling begins to generate locoregional pain.
On my advice, the patient then performs a specialist consultation with Professor Campanacci Andrea Domenico, director of the SODc Oncological and Reconstructive Orthopedics of the Oncology and Robotic Surgery Department of the University Hospital of Careggi, who believes it is advisable to proceed with fine needle aspiration under ultrasound guidance. of the new formation. The histological report documents "skin fragment with notes of fibrosclerosis of the dermal stroma and stromal fragment with minimal cubic lining and myxoid degeneration (histological findings indicative of mucoid-cystic degeneration of the stroma)". The patient is then operated on (excisional biopsy) with eradicating intent. About six months after the operation, however, the patient returns to my ultrasound clinic with a new small internal retromalleolar swelling in the region of the surgical scar. Unfortunately I am going to document a recurrence of the dermal mucoid cyst, with a simple anechoic content.